Lindsey and I met with the surgeon for a pre-op consultation. All in all kind of a waste of time, but whatever. The one thing that was decided was a surgery date. Jan. 25th will be the date I lose about a third of my large intestine. Oh and what ever is left of the cancer. Why do I say what ever is left? Well I guess 25% of the time the cancer is completely killed by the radiation and when they take it out. Which in the end doesn't mean the treatment changes (still will have surgery to remove it and chemo to kill whatever may be floating around my body), but the down staging of the tumor reduces the chance of recurrence and in the end that's the main goal of this whole thing. I can tell right now that the tumor is smaller, how can I tell. Well besides the fact that bowel movements feel like passing fireballs currently, they are about twice the diameter as they were at the beginning of this whole thing. So, the tumor that was clogging the pipes isn't doing much clogging anymore, which is phenomenal. You take for granted how great taking a complete and full bowel movement is, until you can't.
So it looks like I'll be in the hospital for 3-5 days. I can't leave until my bowel 'wakes up' and they need to make sure there's no leakage in the anastomosis (the reconnection of the bowel). Surprisingly I'm suppose to take walks as it helps 'wake up' the bowel and I can eat, when I feel like eating.
As of now I don't have any cancer related appointments until the 14th of Jan. for CT and PET scans, then a colonoscopy on the 16th. So three weeks without having to go to Stanford to get poked and prodded at, sweet. On top of that I'm feeling better everyday (pain in my a**, is almost not a pain any longer...for now), so the holidays should be pretty enjoyable.

Sunday, December 23, 2012
Thursday, December 6, 2012
Pain in Nick's A**: FIRE IN THE HOLE!!
Anyone who loves pickled jalapenos (when I say love I mean 1-2 pickled jalapenos per nacho chip for a good size serving of nachos or equivalent) like I do, has experienced a little of what I'm going through. I OD'd once on pickled jalapenos, not pleasant, not as bad as the night I OD'd on garlic (yes it's possible...oh is it possible)...but that's another story. Anyways, take the next day's pickled jalapeno bowel movement and multiply that by 10, then have the 10 slowly decline over the next 2-3 hours. That's about what a 5th week of radiation therapy to the rectal area, bowel movement feels like. Needless to say pickled jalapenos have not graced my dinner plate in some time, no need to add insult to injury.
I was prescribed what they call butt balm (Nystatin, Lidociane, Desitin in equal parts) to slather on like diaper rash cream (which I'm now a pro at with Oliver's sensitive booty skin). It seems to work OK. I will say that the saving grace has been the Cottonelle flush-able wipes, because wiping with dry TP these days feels like wiping with 60 grit sand paper.
All in all I'm still feeling pretty good. Met with the Radiation Oncologist on Monday and he said I'm their new model patient, as I'm still working and feeling pretty good. I guess the model patient prior to me was only able to handle working 3/4 of the way through treatment. I do have to say that part of me feeling so well has been my beautiful wife taking such good care of me. The symptoms prior to the start of treatment were pretty damn uncomfortable (basically feeling like you have to take a s**t (sorry couldn't bring myself to say bowel movement one more time) all day, then you do and the feeling comes back 10 mins later) and those are all but gone. So from a bowel comfort level I feel much better today than I did day one. More than anything I just feel super tired and sick from time to time, but that's pretty easy to contain.
One more trip under the radiation gun and 10 more chemo pills and Phase 1 is complete. Still a long road ahead, but looking forward to feeling somewhat normal over the Holidays.
I was prescribed what they call butt balm (Nystatin, Lidociane, Desitin in equal parts) to slather on like diaper rash cream (which I'm now a pro at with Oliver's sensitive booty skin). It seems to work OK. I will say that the saving grace has been the Cottonelle flush-able wipes, because wiping with dry TP these days feels like wiping with 60 grit sand paper.
All in all I'm still feeling pretty good. Met with the Radiation Oncologist on Monday and he said I'm their new model patient, as I'm still working and feeling pretty good. I guess the model patient prior to me was only able to handle working 3/4 of the way through treatment. I do have to say that part of me feeling so well has been my beautiful wife taking such good care of me. The symptoms prior to the start of treatment were pretty damn uncomfortable (basically feeling like you have to take a s**t (sorry couldn't bring myself to say bowel movement one more time) all day, then you do and the feeling comes back 10 mins later) and those are all but gone. So from a bowel comfort level I feel much better today than I did day one. More than anything I just feel super tired and sick from time to time, but that's pretty easy to contain.
One more trip under the radiation gun and 10 more chemo pills and Phase 1 is complete. Still a long road ahead, but looking forward to feeling somewhat normal over the Holidays.
Here comes trouble!!
Well Oliver's curiosity of all things continues to grow. He's getting stronger, taller, and smarter which makes containing him more difficult. Our philosophy is to not let him do something that will do major harm (bumps and bruises are part of growing up), but let him explore the limits. He's tried to climb the bar stools twice now, both ended in failure. The other day he grabbed his toy microwave and pushed it up to the wall then proceeded to climb on top of it to reach the light switches.

I was watching the whole thing, decided he couldn't kill himself and let it proceed. Overall he's a pretty cautious climber and will fuss when he feels he gets 'stuck'. Then a proceed to tell him, "you got yourself into the mess, get yourself out." 9 times out of 10 he figures it out, that 10th time usually requires a 'spot'.
He's also figured out the water dispenser on the fridge. Luckily, we've gated the kitchen so we can keep him out most of the time. Otherwise there would be a puddle on the ground all the time because he absolutely loves playing with water. From time to time Lindsey or I will forget the gate is open. Of course he takes advantage of that, by running in there, slamming the gate behind him, turning to us to wave and say, "buh -bye", then proceed to make trouble.

As you can see we're not raising an idiot. I mean if you're going to play with water why would you not have a kitchen towel handy to dry yourself off from time to time. It only makes logical sense.

Oliver playing with the light switch.
I was watching the whole thing, decided he couldn't kill himself and let it proceed. Overall he's a pretty cautious climber and will fuss when he feels he gets 'stuck'. Then a proceed to tell him, "you got yourself into the mess, get yourself out." 9 times out of 10 he figures it out, that 10th time usually requires a 'spot'.
He's also figured out the water dispenser on the fridge. Luckily, we've gated the kitchen so we can keep him out most of the time. Otherwise there would be a puddle on the ground all the time because he absolutely loves playing with water. From time to time Lindsey or I will forget the gate is open. Of course he takes advantage of that, by running in there, slamming the gate behind him, turning to us to wave and say, "buh -bye", then proceed to make trouble.

Playing with the wa wa dispenser.
As you can see we're not raising an idiot. I mean if you're going to play with water why would you not have a kitchen towel handy to dry yourself off from time to time. It only makes logical sense.
Monday, December 3, 2012
Pain in Nick's A**: Radiation Therapy
So lets talk about radiation therapy. Why radiation therapy? Because I think it's kind of cool. Well the radiation portion isn't that cool, it's pretty straight forward. Shoot tumor with radiation, tumor starts to die. Simple right. The trick is how to deliver the radiation dose to the tumor while trying to spare the surrounding tissue as much as possible. There are some things that's you'd rather not shoot with radiation if you don't have to. Those of us of child bearing age, would prefer to keep the family jewels intact. The bladder and prostate seem to be important things, shooting them with radiation is probably not a good idea. With that said, the cancer will kill you dead, so maybe a little radiation damage to the prostate is acceptable. But how do you minimize the damage to the surrounding tissues, while providing enough of a kill shot to the tumor?
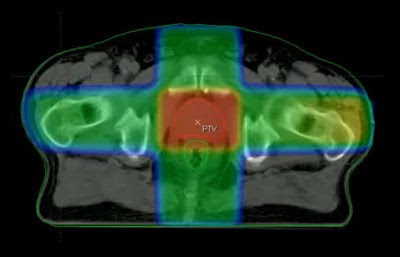
Radiation therapy it the medical use of ionizing radiation to damage the DNA of the cancer cells so that they die and/or slow the reproduction. In the old days, the machines typically shot radiation in 4 directions. They'd shoot you from A (anterior) to P (posterior) (front to back). Then they moved the machine 90 degrees and shoot laterally across your body. Then move the machine 90 more degrees and shoot P to A (back to front) and finally move another 90 degrees and shoot you laterally the other direction. The problem with this is you only distribute the radiation dose across 4 different shots, so a higher radiation dose is delivered to healthy tissue. The dose distribution map for this older method, below.
The next advance seems to have come from IMRT (Intensity Modulated Radiation Therapy) The idea here is not only does a patient get shot at from more angles, but the beam is also modulated in shape to more precisely target the tumor. The dose distribution map for this method, below.

As you can see from the above two fields the IMRT targets the tumor more precisely and while more healthy tissue gets radiated, it is getting a much smaller percentage of the total dose. The below video does a good job explaining IMRT and how the 'shutters' shape the dose.
They have now taken it a step further. If multiple beams are better why not just shoot radiation at the tumor while the 'gun' is dynamically moving around the patient. This is a technology developed by a local Bay Area company called Varian Medical Systems and they call the technology Rapid Arc. It basically allows more precise targeting with more healthy tissue being spared. Below is a quick video describing it.
I'm being treated on a Varian Clinac 21EX with all of the upgrades. The upgrades include Rapid Arc as well as an on-board imaging system capable of both x-rays and CT scans. Below is a picture of the machine that's doing the work.

My treatments start out by me lying on the couch (bed with the sheet), then the techs position me by moving both me and the couch (couch is capable of moving in 3 directions and rotation in one) to align the tattoos on my torso (yes, I have some tats now cause I'm hard core...actually just three <1mm dots) with lasers. Below is a pic of me in position.

Once positioned on the couch everyone except me leaves the room. The techs proceed to take both an A-P and a lateral x-ray. On Mondays they also include a CT scan. After the scans are taken they make some final adjustments (adjustments are made to 0.1cm or 1mm) to my location and the treatment starts. The treatment lasts about 2 minutes as the 'gun' encircles me twice (I don't feel a thing as they're shooting me), then I'm done. The daily radiation dose is 2 Gy for a total of 50 Gy for all 25 days. The whole appointment from when I'm called back to finished is probably less than 10 minutes.
Radiation therapy it the medical use of ionizing radiation to damage the DNA of the cancer cells so that they die and/or slow the reproduction. In the old days, the machines typically shot radiation in 4 directions. They'd shoot you from A (anterior) to P (posterior) (front to back). Then they moved the machine 90 degrees and shoot laterally across your body. Then move the machine 90 more degrees and shoot P to A (back to front) and finally move another 90 degrees and shoot you laterally the other direction. The problem with this is you only distribute the radiation dose across 4 different shots, so a higher radiation dose is delivered to healthy tissue. The dose distribution map for this older method, below.

Conformal Radiotherapy dose distribution field
The next advance seems to have come from IMRT (Intensity Modulated Radiation Therapy) The idea here is not only does a patient get shot at from more angles, but the beam is also modulated in shape to more precisely target the tumor. The dose distribution map for this method, below.

IMRT dose distribution field
As you can see from the above two fields the IMRT targets the tumor more precisely and while more healthy tissue gets radiated, it is getting a much smaller percentage of the total dose. The below video does a good job explaining IMRT and how the 'shutters' shape the dose.
IMRT Video
They have now taken it a step further. If multiple beams are better why not just shoot radiation at the tumor while the 'gun' is dynamically moving around the patient. This is a technology developed by a local Bay Area company called Varian Medical Systems and they call the technology Rapid Arc. It basically allows more precise targeting with more healthy tissue being spared. Below is a quick video describing it.
Rapid Arc Video
I'm being treated on a Varian Clinac 21EX with all of the upgrades. The upgrades include Rapid Arc as well as an on-board imaging system capable of both x-rays and CT scans. Below is a picture of the machine that's doing the work.

Varian Clinac 21EX at the Stanford Cancer Center
My treatments start out by me lying on the couch (bed with the sheet), then the techs position me by moving both me and the couch (couch is capable of moving in 3 directions and rotation in one) to align the tattoos on my torso (yes, I have some tats now cause I'm hard core...actually just three <1mm dots) with lasers. Below is a pic of me in position.

Positioned and ready to go
Once positioned on the couch everyone except me leaves the room. The techs proceed to take both an A-P and a lateral x-ray. On Mondays they also include a CT scan. After the scans are taken they make some final adjustments (adjustments are made to 0.1cm or 1mm) to my location and the treatment starts. The treatment lasts about 2 minutes as the 'gun' encircles me twice (I don't feel a thing as they're shooting me), then I'm done. The daily radiation dose is 2 Gy for a total of 50 Gy for all 25 days. The whole appointment from when I'm called back to finished is probably less than 10 minutes.
Subscribe to:
Posts (Atom)